Asthma is a chronic (long term) inflammatory lung disease which leads to constriction (narrowing) of the airways. It is not known why this inflammation develops but asthma tends to be more common in those with a family history of asthma, children whose parents were smokers and also in those with a past history of allergic disorders such as hayfever and eczema. It's likely therefore that genetic factors combined with certain environmental factors influences whether or not someone develops asthma. According to 'Asthma UK', 1 in 11 children and 1 in 12 adults suffer from asthma in the UK. Asthma can start at any age but most commonly starts in childhood. Asthma is not currently preventable or curable, but it is controllable and most people who have it can lead active and relatively normal lives.
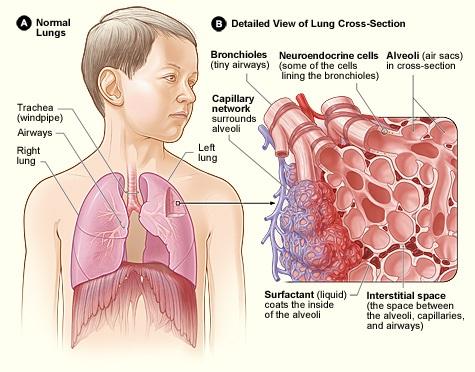
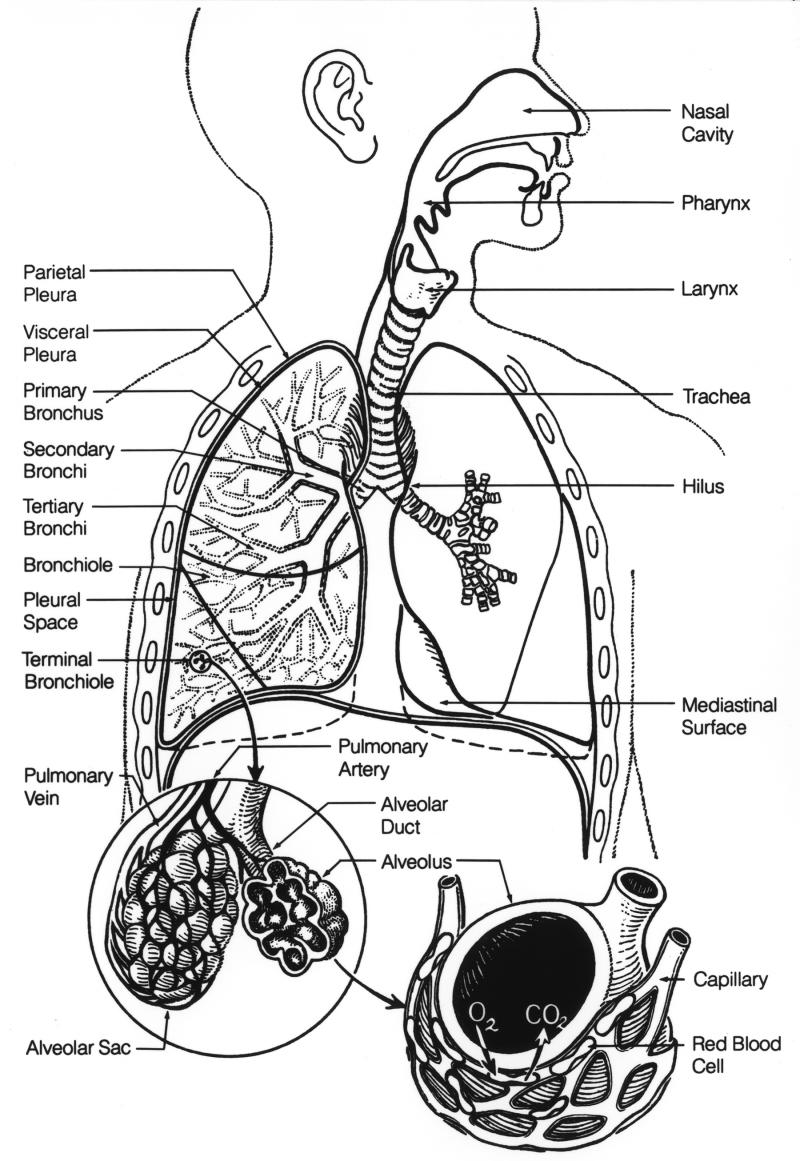
Asthma is a disease of the airways. The airways in our lungs are composed of tubes called bronchi and bronchioles. Bronchi are muscular tubes that carry air throughout the lungs, transporting it to and from smaller airway branches called bronchioles. Asthma affects these smaller tubes (bronchioles) by causing inflammation within the tubes. This causes the walls of the bronchioles to swell and produce extra fluid (mucus), which narrows the airway and makes it more difficult to breathe. Asthma also causes the muscles around the bronchioles to constrict which in turn narrows the airways further. The combination of these factors can cause a cough, wheeze or shortness of breath which are the main symptoms of asthma.
These symptoms may vary in severity depending on how bad the narrowing in the airways is and how long it lasts for, and asthma affects people to different extents. If the narrowing in the airways is quite severe this may result in an asthma attack where the person finds it quite difficult to breathe as very little air can flow along the airways. The attack may be so severe that the person needs to be admitted to hospital or even be put on a ventilator to help them breathe. At other times during an attack the airways may be less narrow and the person may have mild symptoms such as a cough or a slight wheeze. It is thought that there are certain “triggers” which irritate the airways and cause the symptoms of asthma. Everyone's asthma is different and a person may have several triggers. However a lot of the triggers for asthma are due to people being allergic to particular substances which are called allergens. Asthma attacks can be triggered in these people if they come into contact with these substances. In these patients the airways over-react to allergens in the air such as pollen, pollution, mould, dust mites, animals, particles, and fumes and this causes the airways to constrict and become inflamed. Asthma attacks may also be caused by other triggers such as stress, strong emotional responses (laughing, crying, and anger), exercise, viral infections, and cold air. Sometimes asthma can be triggered by dust or fumes at work (‘occupational asthma’), for example people who work in chemical processing, food processing, metal work, spray painting, woodwork or farming. Medicines such as beta-blockers, aspirin and ibuprofen can also trigger attacks. Rarely, sulfites found in wine and dried fruit can cause episodes of asthma in some people. Asthma attacks can occur at any time but are especially frequent at night and in the morning.Inhalers are used to treat asthma and work by opening up the airways making it easier to breathe. This is usually by relaxing the muscles around the airways so that they open up (usually called a “reliever inhaler” e.g Ventolin). Other inhalers, such as steroid inhalers, work by reducing the inflammation in the airways that caused it to narrow in the first place. This effect is not immediate however and it takes some time for the inflammation to reduce. Because of this, these sorts of inhalers are usually used regularly to prevent asthma attacks and do not work to relieve an acute attack. Steroid tablets however also work in a similar way, and are often used for a short while together with inhalers in patients who are having a severe exacerbation (worsening) of their asthma. Although the effects are not immediate, they often help to reduce inflammation within a day or so reducing the risk of a severe attack that may require hospitalisation. They can also be used regularly as a preventative treatment in patients with extremely severe or uncontrolled symptoms. As the severity of asthma will differ for different people, some people will only need to use reliever inhalers. Others may need to use a preventer inhaler as they have regular attacks and those with really severe symptoms may be on long term oral steroids. Other oral medications may also be used in asthma. Montelukast is a tablet that blocks the effect on the airways of a substance called leukotriene, which causes inflammation in the airways. Another medication called theophylline works on relaxing the muscles around the airways.
It is important you know how and when to take your medications, and when to seek medical attention. Your GP may give you written instructions (‘asthma action plans’) which can help you to take control of your own asthma. Asthma reviews help you make sure that you are getting the right treatment and that you know how to use your inhalers properly. If you are a smoker then one of the best things you can do to help your asthma, or your childs asthma, is to stop smoking.