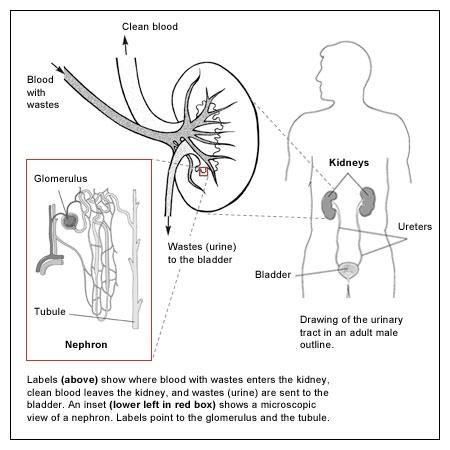
The kidneys are part of the body's urinary tract. The urinary tract consists of two kidneys, two tube-like ureters that drain urine from each kidney into the bladder (a storage sac), and the urethra, another tube that carries the urine out of the body. Muscles control the release of urine from the bladder.
The kidneys are a pair of bean-shaped organs that are located at the bottom of the ribcage in the right and left sides of the back. Within them are about a million tiny functional units called nephrons. At the beginning of each nephron, blood is continually filtered through a microscopic cluster of looping blood vessels, called a glomerulus. The glomerulus allows the passage of water and small molecules but retains blood cells and larger molecules. From the glomerulus the fluid and molecules pass into the proximal tubule, the Loop of Henle, the distal tubule and then the collecting ducts. During this journey the waste products are concentrated to make urine while simultaneously products that the body still can use will be reabsorbed.
The kidneys control the quantity and quality of fluids within the body. They also produce: Erythropoietin (EPO), which stimulates the bone marrow to make red blood cells; Renin, which helps control blood pressure; Calcitriol, the active form of vitamin D, which is needed to maintain calcium for teeth and bones and for normal chemical balance in the body.
Among the important molecules that the kidneys help to regulate are sodium, potassium, chloride, bicarbonate, calcium, phosphorus, and magnesium. The right balance of these substances is critical. When the kidneys are not working properly, waste products and fluid can build up to dangerous levels in the blood, creating a potentially life-threatening situation.
Although the body is equipped with two kidneys, it can function with one reasonably healthy kidney if the other is damaged or removed. However, when kidney – or "renal" – function drops below 25% (people with two healthy kidneys have 100% of their kidney function), serious health problems can occur, and when function drops below 10-15%, critical intervention in the form of dialysis or kidney transplantation becomes necessary to maintain life. This is called end stage renal disease (ESRD or kidney failure).
A sudden loss of kidney function, over a few hours or days, is called acute kidney injury (AKI, formerly called acute renal failure or ARF). When kidney damage and decreased function occurs over time and/or lasts longer than 3 months, it is called chronic kidney disease (CKD). The next page of this article provides information on some of the causes of these conditions.