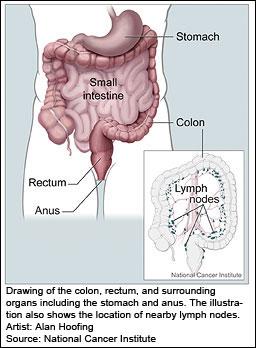
The bowel forms part of the digestive system and is divided into two parts, the small bowel and the large bowel. The large bowel is made up of the colon and rectum; the colon makes up most of the 5 foot length of the large bowel.
Food passes from the stomach to the small bowel. After the small bowel takes nutrients into the body, any undigested food passes through the large bowel, where water is removed from the waste matter.
Bowel cancer is also known as colon, rectal or colorectal cancer. Bowel cancer is the third most common cancer in the UK, after lung and breast cancer. It is the second most common cause of cancer death, after lung cancer. Approximately 95% of all diagnoses are in people over the age of 50. Most cases of bowel cancer begin with the development of benign polyps, finger-like growths that protrude into the intestinal cavity. These benign polyps are not cancer and relatively common in people over age 50. They can become cancerous though, with the ability to invade the normal bowel and spread to other parts of the body (metastasize). The tumours can create blockages in the intestine, preventing elimination.
The exact causes of bowel cancer are not known, but risk appears to be associated with genetic, dietary, and lifestyle factors. Those with a personal or family history of bowel cancer or polyps are at a higher risk, as are those with ulcerative colitis, inflammatory bowel disease, and immunodeficiency disorders. A very rare inherited disease, called Familial Adenomatous Polyposis (FAP), causes benign polyps to develop early in life and cancer develops in almost all affected persons unless the colon is removed. Another genetic condition called Hereditary Non-polyposis Colorectal Cancer (HNPCC) accounts for around 2-5% of cases of bowel cancer. Polyps develop at a younger age and at a greater frequency than in individuals who do not have the disease, but not in such large numbers as FAP.
The risk of bowel cancer increases with age and with the occurrence of cancers in other parts of the body. High fat and high meat diets are risk factors, especially when combined with minimal fruit, vegetable, and fibre intake. Lifestyle risk factors include cigarette smoking, obesity, and a sedentary lifestyle.